Another name for Gynecologic Carcinosarcoma (GCS) is malignant mixed Müllerian tumor (MMMT), an older term that is still being used.
Gynecologic Carcinosarcoma is a cancerous growth found in the uterus, ovaries, cervix, vagina, fallopian tubes and other parts of the body. 1
Carcinosarcoma is unique in that it contains both carcinomatous (malignant epithelial tissue) and sarcomatous (mesenchymal or connective tissue) components. The sarcomatous component may be either homologous (made of tissue normally found in the organ) or heterologous (made of tissue not normally found in the organ). 2
GCS is rare. Very rare. Fewer than 1,000 cases of GCS are diagnosed each year. Carcinosarcoma accounts for less than 5% of uterine cancers and less than 1-4 % of ovarian cancers.3, 4
Because of its rarity, the small number of cases has prevented large studies and trials that are necessary to evaluate various treatments. 1, 2
GCS occurs predominantly in postmenopausal women with an average age of 66 years.
Risk factors include never having given birth (nulliparity), advanced age, obesity, external sources of estrogens (such as estrogen replacement therapy), and long-term use of tamoxifen.1
“Tamoxifen is associated with a 2–7x greater risk of developing endometrial malignancies. Specifically, carcinosarcomas have been reported to occur 7–20 (median of 9 years) years after the initiation of this regime. On the contrary, oral contraceptives are reported to provide a protective effect against these tumors.” 1
GCS is highly aggressive and often has metastasized (spread) to other parts of the body by the time of diagnosis; 60% of patients with uterine carcinosarcoma and 90% of patients with ovarian carcinosarcoma have metastasis by the time of diagnosis.1, 2
How is Uterine or Ovarian Carcinosarcoma Treated?
New breakthroughs in immunotherapy and personalized cancer treatments are being discovered every day. Because GCS is so rare, it is not on the radar screen for these new therapies. But this is where the cures will be found. The current therapies — surgery, radiation and chemotherapy — have not yielded any improvement in survival in over 40 years.
As of today, there are no consensus guidelines for the treatment of GCS. GCS is so rare that it has not been studied as a unique entity. Instead, it has been treated as an ovarian cancer or uterine cancer with poor results. What we are learning is that the carcinomatous and sarcomatous components of carcinosarcoma respond differently to chemotherapy.
Writing about uterine carcinosarcoma, Kanthan and Senger state that “a full understanding of the pathobiogenesis of this tumor is necessary to predict the “gold standard” treatment.”1 This is where The GCS Project is making its initial impact. Read about the ground-breaking research that we initiated, which involves extensive genetic analysis of carcinosarcoma tissue specimens to discover tumor mutations that can be targets for drug therapies to treat and cure the disease!
In many cases, surgery is the first treatment for GCS. Chemotherapy, as an adjuvant (additional) treatment is also necessary to manage recurrence and metastasis following surgery.
In more advanced disease, Kanthan and Senger note that “neither radiotherapy nor chemotherapy provides any significant overall survival benefit, and there remains to date no consensus to guide therapeutic strategies for the various stages of disease.”1
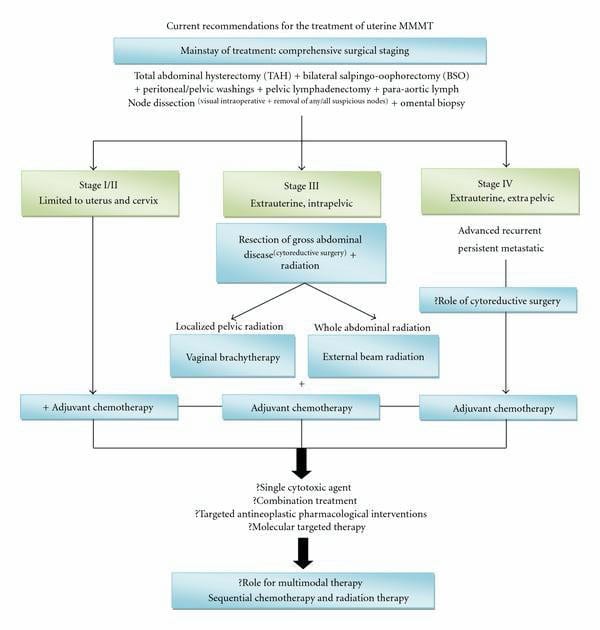
I found this flow chart1, which summarizes the current recommendations for the treatment of uterine carcinosarcomas. (Source)
Newly Diagnosed?
Take a look at our Resources page for information you’ll want to read and steps you’ll want to take.
Kanthan, R., & Senger, J-L. Uterine carcinosarcomas (malignant mixed mullerian tumours): A review with special emphasis on the controversies in management. Obstetrics and Gynecology International, 1-13. doi:10.1155/2011/470795
Del Carmen, M. G., Birrer, M., Schorge, J. O. Carcinosarcoma of the ovary: A review of the literature. Gynecologic Oncology,125, 271-277. ( View PDF)
Berton-Rigaud, D., Devouassoux-Shisheboran, M., Ledermann, J.A., Leitao, M. M., Powell, M. A., Poveda, A., . . . Ray-Coquard, I. Gynecologic cancer intergroup (GCIG) consensus review for uterine and ovarian carcinosarcoma. International Journal of Gynecological Cancer, 24(S3), S55-S60.
Penson, R. T., & Powell, M. A. Clinical features, diagnosis, staging, and treatment of uterine carcinosarcoma. In S. J. Falk (Ed.), ( View Source )
Clinical trials are currently being offered at the University of Arkansas for Medical Sciences (UAMS). Phase 1/2 Study to Evaluate the Safety, Pharmacokinetics, and Efficacy of BLU-222 as a Single… Read More »
Clinical trials are currently being offered at the University of Alabama at Birmingham. Immunotherapy has gained a significant amount of attention recently, but its efficacy as a single agent in… Read More »
Clinical trials are currently being offered at Medical University of South Carolina (MUSC) Health Care in Charleston SC. A Phase II/III Study of Paciltaxel/Carboplatin alone, or combined with either Trastuzumab… Read More »